Thyroid gland
The thyroid gland is an very important hormone secreting gland in endocrine systems, it is 2-inch-long, butterfly-shaped consists of two bulky lateral lobes connected by a relatively thin isthmus, usually located below and anterior to the larynx. It is one of the glands that make up the endocrine system. Thyroid follicular epithelial cells convert thyroglobulin into thyroxine (T4) and lesser amounts oftriiodothyronine (T3). T4 and T3 are released into the systemic circulation. The binding proteins serve to maintain the serum unbound ("free") T3 and T4 concentrations within narrow limits yet ensure that the hormones are readily available to the tissues.
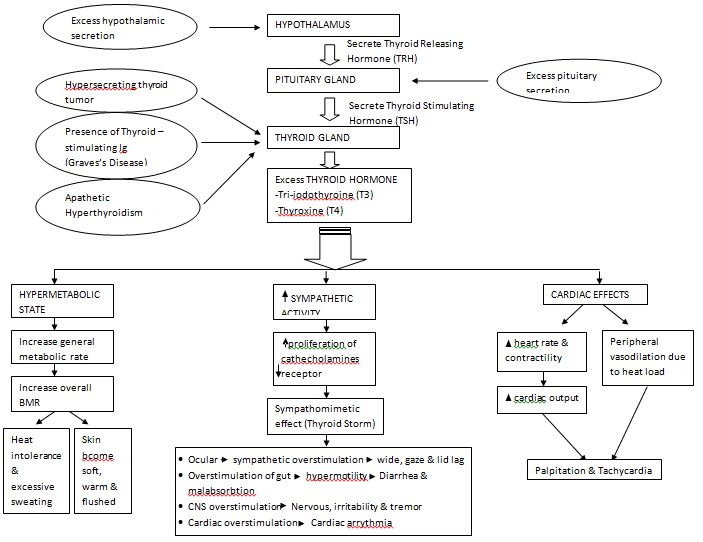
According to Dorland's medical dictionary, Hyperthyroidism is defined as an excessive thyroid gland activity, marked by an increased metabolic rate, goiter, and disturbance in autonomic nervous system and in creatine metabolism. It is a hypermetabolic state caused by elevated circulating levels of free T3 and T4, most commonly by abnormal increased function of the thyroid gland. However, in certain conditions the oversupply is related to either excessive release of preformed thyroid hormone or to an extra-thyroidal source.
Thyroid hormones affect metabolism, brain development, breathing, heart and nervous system functions, body temperature, muscle strength, skin dryness, menstrual cycles, weight, and cholesterol levels.
Many common symptoms and signs of increased thyroid hormone (hyperthyroidism) are similar to those of adrenergic excess, such as nervousness, palpitations, hyperactivity, increased sweating, heat hypersensitivity, fatigue, increased appetite, weight loss, insomnia, weakness, and frequent bowel movements (occasionally diarrhea).
Hyperthyroidism has several causes, including:
· Graves' disease (toxic diffuse goiter)
· Inappropriate TSH secretion
· Molar pregnancy, choriocarcinoma, and hyperemesis gravidarum
· Nonautoimmune autosomal dominant hyperthyroidism
· Toxic solitary or multinodular goiter (Plummer's disease)
· Inflammatory thyroid disease (thyroiditis)
· Drug-induced hyperthyroidism (amiodarone, interferon-α)
· Thyrotoxicosis factitia
· Excess iodine ingestion
· Metastatic thyroid cancer
- Struma ovarii